Debunking Ivermectin: A Complete Guide
Over the last year, I’ve watched in horror as ivermectin went from a pet theory to a cultish fringe belief and a dangerous “vaccine alternative”. I put together a comprehensive post summarizing the evidence and why it does not support use of ivermectin outside of a clinical trial.
Conflict between in vitro data and pharmacokinetics -
Ivermania began in early 2020, when a group of scientists in Australia found that ivermectin, a widely used anti-parasitic drug, could apparently stop SARS-CoV2 from replicating in vitro. There are always limitations to in vitro studies, but especially in the early days of the pandemic, a repurposed medication to treat COVID19 was an exciting prospect.
Unfortunately, from inception there appears to have been overreach. The original paper that found that ivermectin inhibited viral replication in cell culture used a 5 micromolar concentration. In vivo the drug has a Cmax of about 50 nanomolar. That means that dose that was required in vitro (IC50) is 100x higher than what can actually be achieved in vivo (Cmax). Even using a dose much higher than the safe/approved dose is unlikely to reach the level that was required in vitro.

Orders of magnitude difference between IC50 and Cmax suggests that ivermectin cannot reach a high enough concentration to inhibit viral replication. For a longer explanation see my video here.
There are some studies in cows that suggest that ivermectin may reach higher levels in specific tissues such as lung, but this effect is fairly modest (e.g. a tissue concentration of 0.8 micro molar compared to a plasma level of 0.5 micro molar). Even if tissue levels were double the plasma levels, the tissue level would still be 50x lower than the dose required in vitro. Closer but still far from viable pharmacokinetics.
Indeed, the authors of the original in vitro paper have said repeatedly that they do not think that there is sufficient evidence to support the use of IVM in people outside of clinical trials.
Incredible results of early clinical trials -
Beginning just months into the pandemic there were a few hastily performed human studies of ivermectin. These studies had results that were simply incredible (and I mean this literally, as in “not credible”).
A large observational trial by Surgisphere found a strong association between ivermectin use and COVID survival. A randomized controlled trial by Elegazzar et al found that ivermectin treatment reduced COVID mortality by over 90%. And another RCT by Carvallo et al claimed that ivermectin prophylaxis was 100% effective in preventing SARS-CoV-2 infection in healthcare workers.
These early studies had implausibly large effect sizes, were mostly pre-prints (some such as Elegazzar were never peer reviewed despite being posted for over a year), and all had glaring methodologic flaws such as being non-randomized, having imbalanced allocation, unequal use of corticosteroids, and using HCQ and other disproven therapies as a control group, etc.
Furthermore, several of these studies - including all the ones that demonstrated increased survival with ivermectin - have been found to be fraudulent.
Surgisphere - also notable for fabricating data on a hydroxychloroquine - had their studies retracted from the NEJM and Lancet and went out of business. The Surgisphere ivermectin study, which never made it beyond a pre-print, none-the-less was the basis for several countries to adopt ivermectin into their treatment guidelines.

Implausible Kaplan-Meyer curve from the now retracted Surgisphere manuscript. This is the fraudulent study that kicked off ivermania.
On forensic examination, many more of the studies that had impossibly large benefits appear to have been faked:
The Elegazzar et al RCT, which purported to show a 90% treatment benefit, was withdrawn after the data was shown to be fabricated.
Similarly the Carvallo et al RCT, which showed a huge benefit to ivermectin prophylaxis, appears to have never been performed at all.
Another large study in Brazil, by Cadegiani et al, also appears to have been fabricated.
Finally, the Niaee et al study appears to have not been properly randomized (and is likely also fraudulent). This was the last interventional study that showed a survival benefit to ivermectin in COVID19. Excluding this dubious study, there are now literally zero studies that demonstrate a survival benefit to ivermectin.
Discounting these fabricated studies, the ivermectin literature looks much less incredible.
Higher quality RCTs don’t show benefit to Ivermectin -
This is not to say that all the studies are fake or methodologically flawed. In the last few months there have been some high quality ivermectin RCTs. Examples include the EPIC trial (published in JAMA), IVERCORCOVID (BMJ Infectious Disease), the TOGETHER trial (published in NEJM), the I-TECH trial (published in JAMA Internal Medicine), and ACTIV-6 (currently a pre-print). These more reputable studies have been uniformly negative.
Several ongoing trials should read out soon: PRINCIPLE in the UK and more. We will likely learn more in the coming months. In the meantime, I’d be cautious about interpreting the large number of ongoing trials as evidence of potential benefit, however. Recall that we also did a lot of trials of HCQ after it became popular.
But those trials used too low a dose
When confronted with the ever expanding list of negative RCTs, the ivermectin stans inevitably rejoin that “the dose was too low!" You see the sketchy groups that promote ivermectin have continuously increased the recommended dose:

The FLCCC likes to stay one step ahead of negative trials by constantly increasing the recommended dose & duration of therapy.
For example, back in 2020 (when Pierre Kory testified to congress that ivermectin was a “miracle cure” for COVID) the "recommended dose” for hospitalized patients was just 0.2 mg/kg on days 1 & 3. This is lower than what has been used in everyone of the negative RCTs.
Reputable meta-analyses does not show benefit to ivermectin -
Early in the pandemic there were a few biased narrative reviews and methodologically dubious meta-analyses that supported ivermectin. As the fraudulent studies have been discovered/retracted and as more reputable studies have been completed, there is no longer a signal for benefit in meta-analysis.
This has not stopped a number of anonymous websites, purporting to be “realtime meta-analyses” from claiming that ivermectin is highly effective. These websites, despite superficial polish, cherry-pick secondary endpoints and commit all manner of sophomoric statistical errors.

Note how this dubious “realtime meta-analysis” combines a bunch of totally different cherry-picked secondary outcomes (red box). Also note that size of the study doesn’t affect the weight (blue box); a 1355-person RCT is apparently given the same weight as a 35-person non-randomized study. This is not how meta-analysis works…

Um...Yeah that’s not how probability works...
This illustrates that bad meta-analyses are “garbage in, garbage out.” Appropriate meta-analysis methodology involves performing an initial assessment of quality and risk of bias and may exclude studies that are of low quality. A recent letter to the editor in Nature Medicine described the problem of systemic fraud in the ivermectin literature and suggested that future meta-analysis should always review individual patient data to detect fraud earlier.
It seems that even meta-analyses are not immune to the issue of fraud. Hill et al voluntarily retracted their (previously positive) meta-analysis of ivermectin after the studies it was based on were found to be fraudulent. Kory et al had their review retracted by the journal after it was found to contain inaccurate data showing improved patient survival with their treatment protocol.
As far as definitive summaries of the data go, Cochrane recently performed a meta-analysis and concluded "the reliable evidence available does not support the use of ivermectin for treatment or prevention of COVID‐19.”
Epidemiological studies don’t prove much of anything-
Several “epidemiological studies" purport to show that distribution of ivermectin was immediately followed by declines in ivermectin cases. Indeed, as the literature supporting ivermectin has collapsed, the drug's proponents cling more strongly to these studies purporting to prove benefit. Ivermectin believers often invoke “What about Peru?” or “How do you explain the Uttar Pradesh Miracle?” as catechisms of their faith in ivermectin.
On closer scrutiny these “studies” are really just childishly cherry-picked examples showing COVID spikes followed by declines. In every example, the surge in cases led to numerous proven interventions - lockdowns, testing, contact tracing, mask mandates, vaccination, etc - to which ivermectin was added in desperation. The biological plausibility is questionable: In some cases, ivermectin was given at a low-dose, infrequently (sometimes once a week or less), and to a small fraction of outpatients. In other cases, ivermectin was added to guidelines, but it’s unclear how much was actually distributed.
These studies are inherently non-falsifiable, but common sense can largely debunk the claims made based up on them.
First, the pattern of rapid peak followed by decline is exactly what we saw in areas that are overwhelmed, such as during the tragedies in NY & Italy during the first wave of the pandemic. Ivermectin wasn’t used in either of these cases, but mortality declined rapidly form a high peak. If NYC had started dispensing Nathan’s hotdogs in April 2020, they could have concluded that hot-dogs cure COVID.
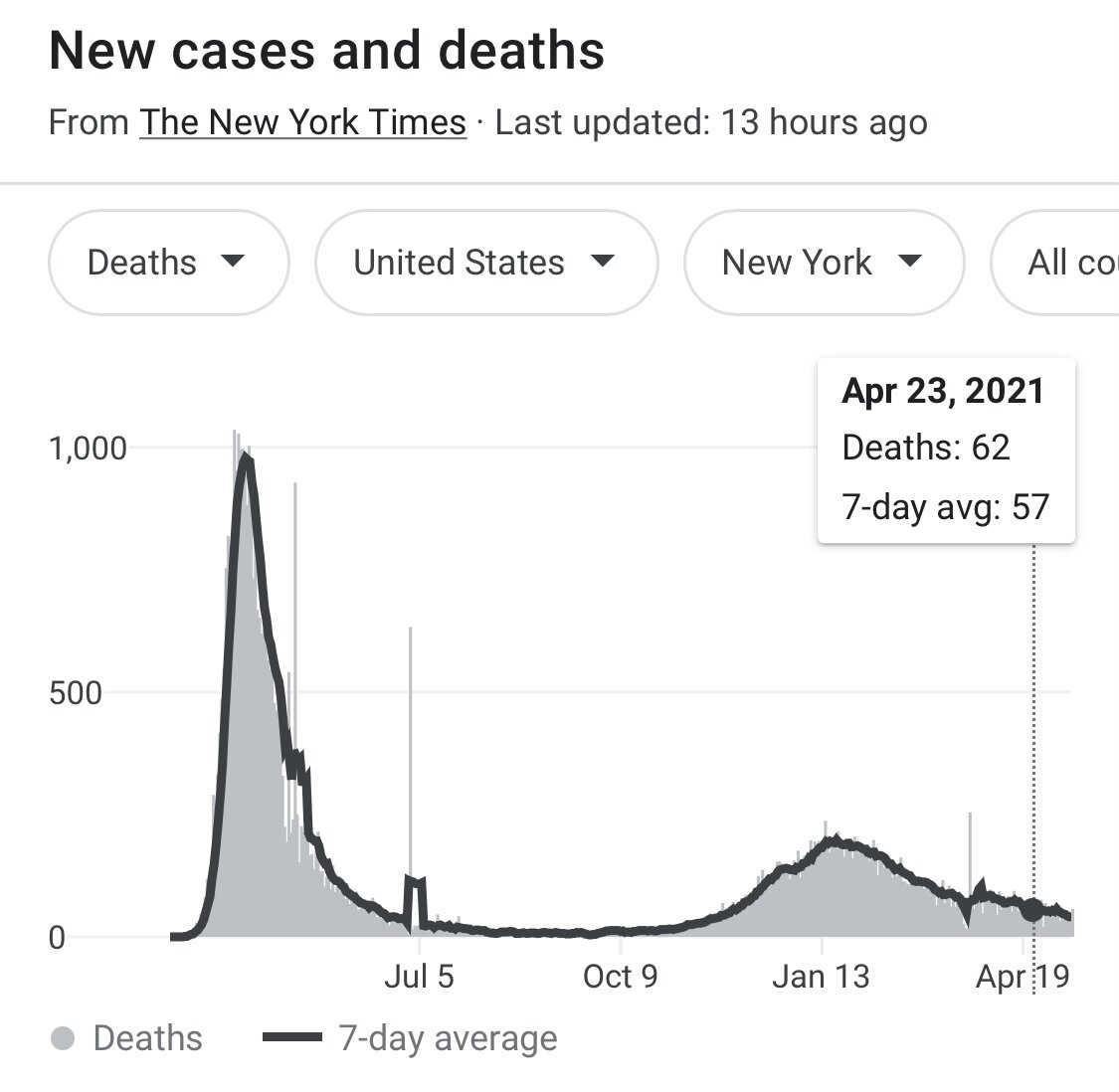
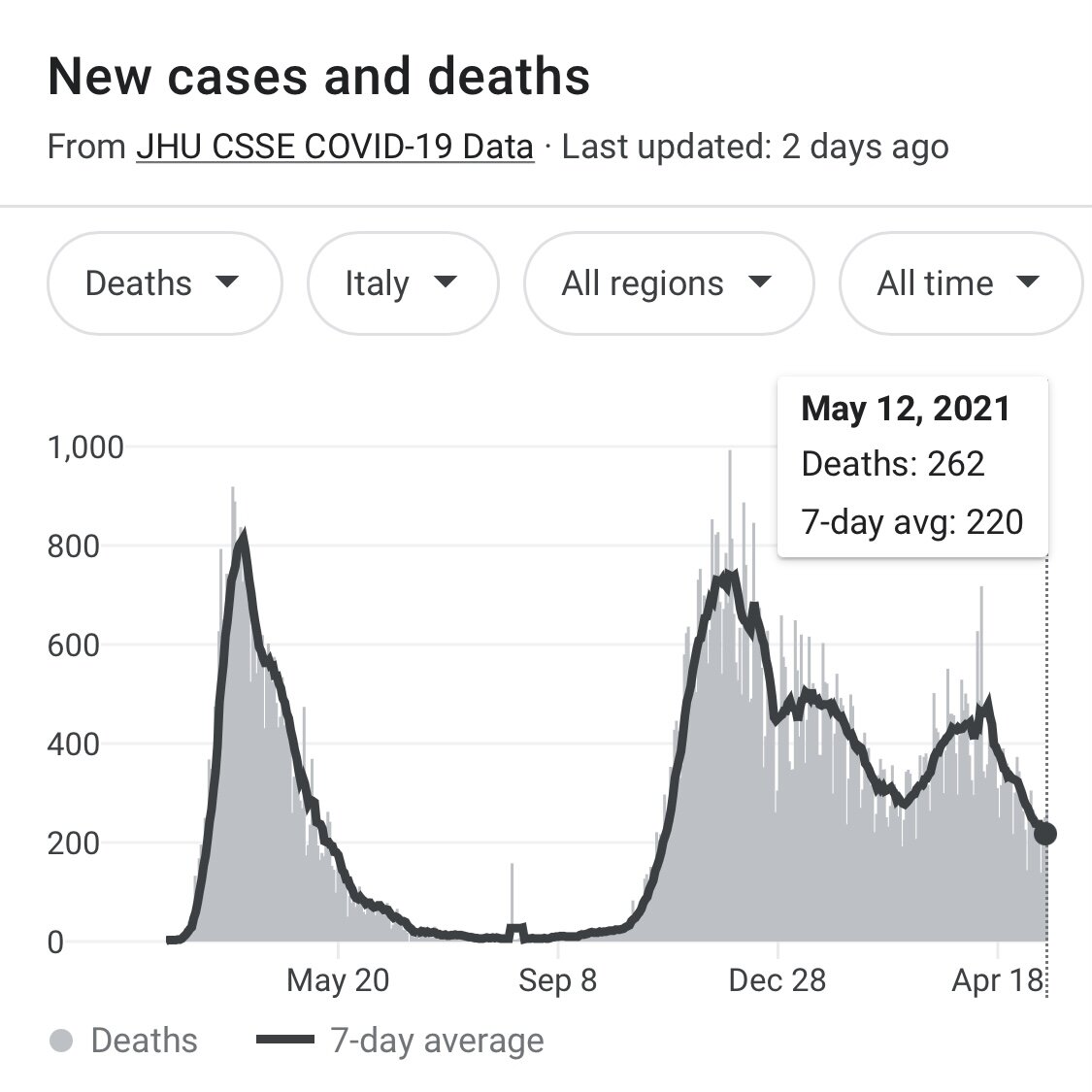
Pattern of mortality after COVID surge in NYC and Italy. Public health interventions (masks, shutdowns/lockdowns, contact tracing, etc) rapidly reduced mortality without any help from ivermectin.
Not only does correlation not equal causation, but in many cases these studies don’t even establish a correlation. Despite claims to the contrary, the distribution of ivermectin in Peru doesn’t seem to be associated with a decrease in COVID cases or deaths.

Dubious epidemiological study from a narrative review, alleging a decline in COVID case before/after ivermectin adoption in Peru.

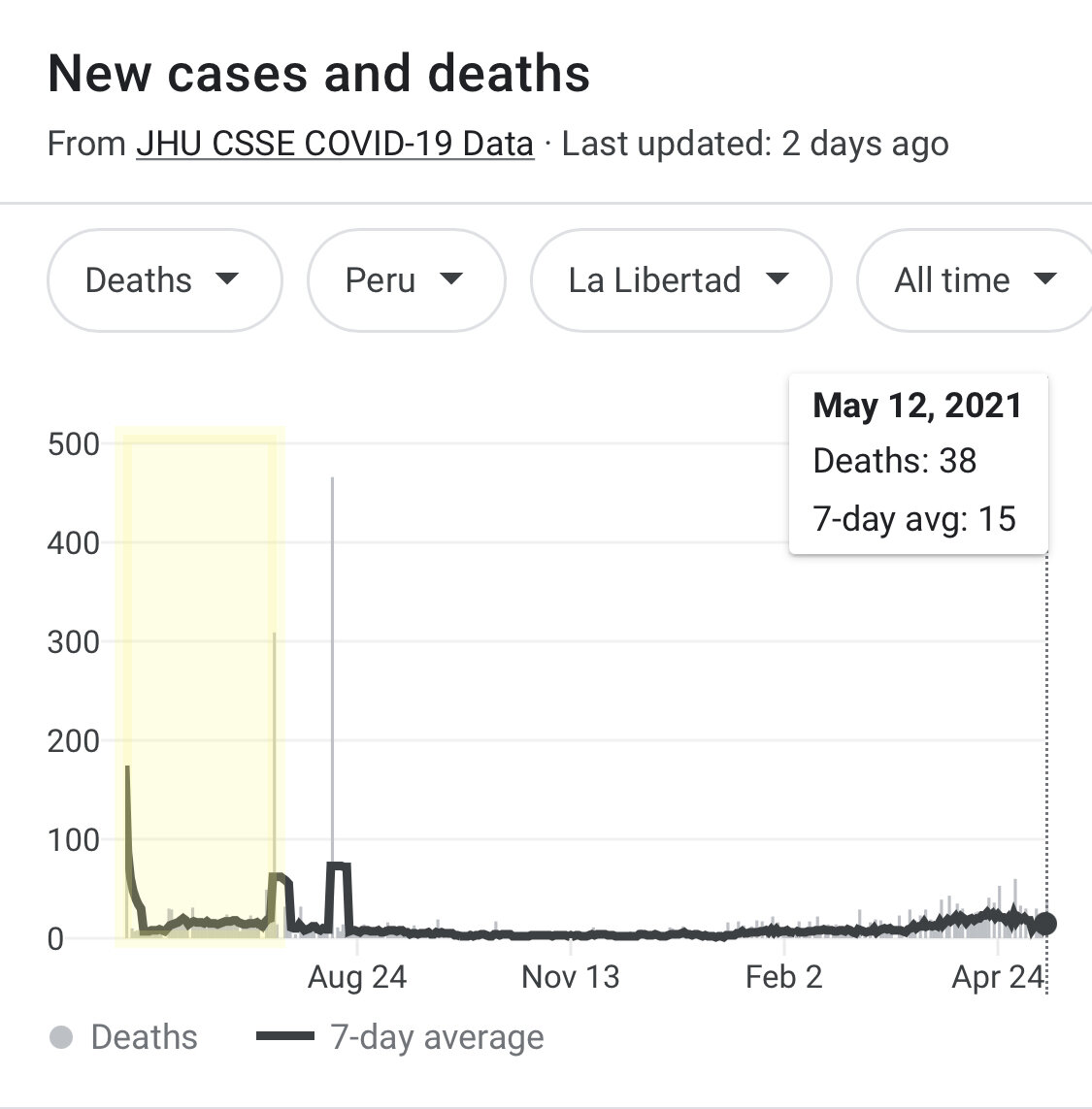
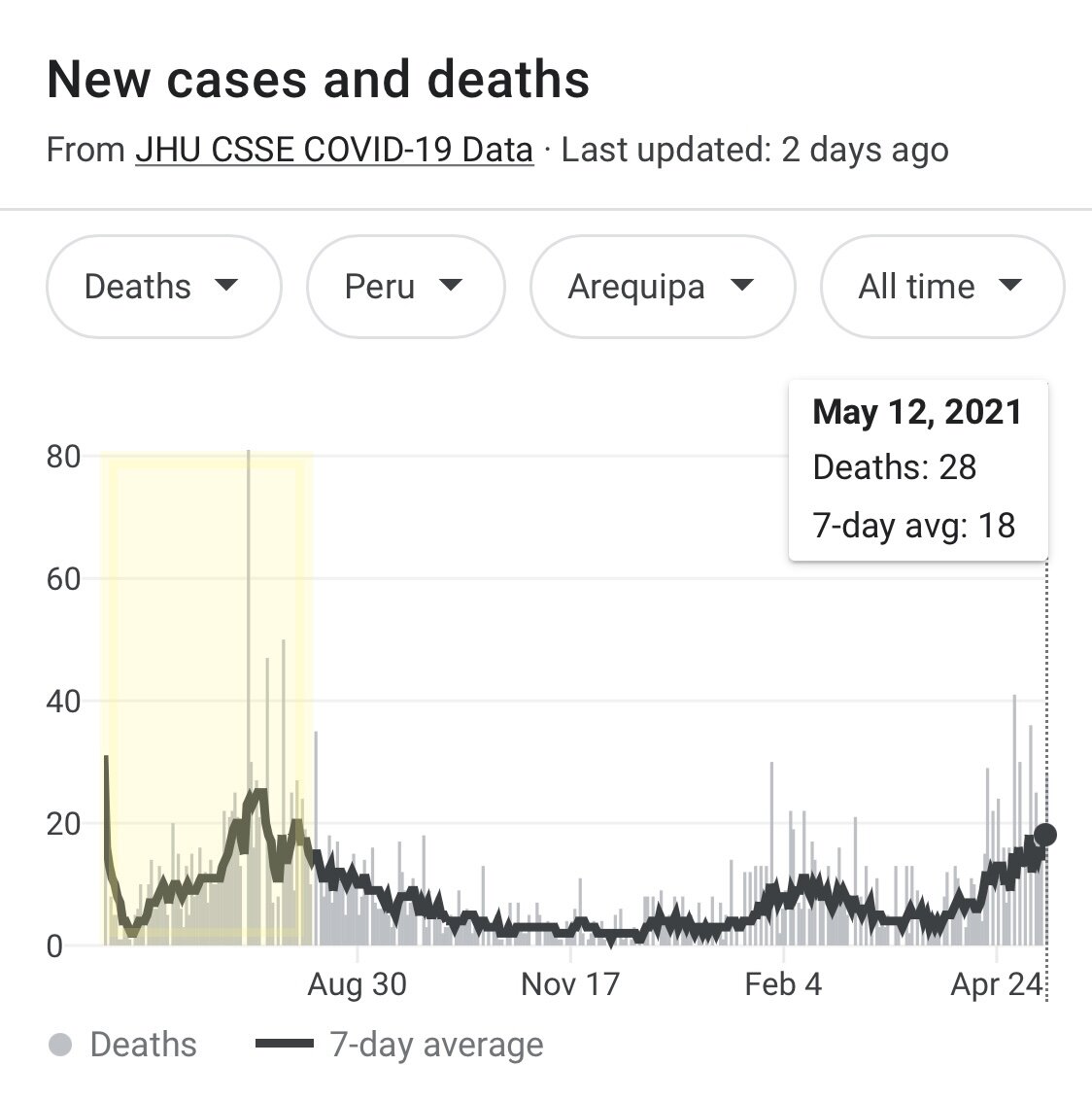

Mortality data for four of the same provinces does not show any signal for benefit, comparing before (yellow box) and after (white) ivermectin was added to treatment protocols.
Peru - As you can see in the figure above, the mortality was already falling in some provinces in Peru when ivermectin was adopted (on May 8, 2020); in other cases mortality rose significantly after adoption. In no case did ivermectin distribution appear to prevent subsequent waves. This is probably why the government of Peru removed ivermectin from their treatment protocols.
Africa - Another bizarre theory is that COVID mortality in Africa has been lower because of pre-pandemic programs that distributed ivermectin to eradicate onchocerciasis (something ivermectin actually does quite well). This theory lacks face validity for at least 3 reasons:
the countries that participate in the African Program for Onchocerciasis Control (APOC) and the Global Programme to Eliminate Lymphatic Filariasis (GPELF) distribute ivermectin ONCE per YEAR. It seems just a bit improbable that a single dose of ivermectin would protect against SARS-CoV-2 infection up to 12 months after taking it.
Unfortunately, many of the programs that distribute ivermectin for control of parasitic worms have been shut down or severely limited due to the pandemic. Thus even if once yearly ivermectin was effective, it hasn’t been given to many people in target countries for up to 2 years.
As Gideon MK (@HealthNerd) argues in this excellent explanatory thread, the more likely explanation for fewer COVID cases in much of Africa is simply under-reporting. Some countries have not reported ANY deaths from COVID.
8/10 We KNOW that the death data in many African countries for COVID-19 is not great. For one thing, some countries simply do not record any COVID-19 deaths (or test for COVID-19 at all)... pic.twitter.com/lTFg0s7eog
— Health Nerd (@GidMK) September 10, 2021
“But what about Uttar Pradesh?!?” If we look at the timing of ivermectin distribution in Uttar Pradesh, India, it seems to be associated with neither ending the alpha variant wave in 2020 nor preventing the delta variant in 2021. This is probably why India also removed ivermectin from their COVID treatment protocols.


Strong work Ivermectin!
It’s worth noting that Uttar Pradesh is an exemplar of evidence-based interventions to control COVID: they had a strict lockdown followed by a curfew, they had a mask mandate (unlike many other Indian states), and they have among the highest vaccination rates in India. It’s also noteworthy that all-cause mortality (not just COVID) is anomalously lower in Uttar Pradesh; there are entire districts in Uttar Pradesh that have literally reported zero deaths from any cause for multiple consecutive months. This suggests that either ivermectin also prevents deaths from cancer and car accidents, or (more likely) that there may be significant underreporting during the pandemic. A recent analysis of public data under the right-to-information law found that the actual mortality was 43 times higher than the officially reported numbers.
Japan - Recently many dark corners of the internet have proclaimed that the decrease in COVID cases in Japan is due to ivermectin. They cite the fact that one official in the Tokyo Medical association proposed using ivermectin at a press conference. This is magical thinking at its finest: there is no evidence that anyone actually prescribed ivermectin after this local press conference. The Japanese government does not recommend using ivermectin & never has. (For a US analogy: Imagine crediting a statement by one guy at a local AMA charter in New York with the sudden decline in cases in Los Angeles or nationwide.)
The “ivermectin saved Japan” theory also conveniently ignores the high rate of vaccination, ubiquitous masking, an effective test/trace program, as well as a fairly restrictive summer lockdown in Japan. Also, as pointed out in an excellent article by @GidMK, the same local non-government official also recommended ivermectin back in February & cases increased afterwards. In fact if you look at trends in COVID cases in the 8 weeks following the actual the press conferences (Feb 9 & Aug 12) it doesn’t appear that ivermectin saved Japan.

Trend in COVID cases in Japan. In two local press conferences on February 9 and August 12, an official with the Tokyo Medical Association recommended ivermectin to treat COVID. In the following 8 weeks COVID cases actually increased in Japan. Data from Our World in Data.
Brazil - Brazil provides a counterpoint to the cherry picked examples above. Despite being an early proponent of ivermectin and widely distributing the drug in “kits,” Brazil was ravaged by COVID in 2020 and 2021. Brazil has highest mortality & the second highest COVID mortality per capita in South America (after Peru). Several of the states in Brazil with the highest self use of ivermectin also had the highest rates of COVID mortality in the world. Furthermore, there are examples of entire towns in Brazil where the population was treated with ivermectin and were subsequently devastated by COVID. This is why, along with Peru and India, Brazil has stopped using ivermectin as part of its COVID treatment protocol.


Despite widespread use of ivermectin in Brazil, the country has among the highest COVID mortality in the world. Like Peru and India, Brazil has stopped using ivermectin to treat COVID. Source: Our World in Data.
No credible group supports the use of ivermectin
Professional & government organizations - no major professional or national body recommends use of ivermectin. NIH, WHO, EMA have all independently looked into IVM and none recommends it outside of a clinical trial. FDA has refused to grant an EUA and is actively recommending against using it in COVID. CDC has also warned against using IVM to treat COVID. Additionally, many other professional organizations such as IDSA, AMA, ASHP, and APhA recommend against using ivermectin to treat COVID19.
Large US Health systems - many health systems have also looked into using ivermectin. Several large health systems (Aurora Health) have gone so far as to ban the use of ivermectin in treating COVID due to a lack of evidence of safety and efficacy. I'm not aware of any US health system that has a policy of treating with ivermectin.
Groups & individuals that support ivermectin are sketchy
Many of the proponents of ivermectin for COVID are more than a little sketchy. The two organizations in the US - America's Frontline Doctors & Frontline COVID Critical Care Alliance (FLCCC) - take money from & are affiliated with anti-vax causes. Both present ivermectin as a "vaccine alternative.” America’s Frontline Doctors grifted over $6.7m from patients seeking ivermectin, and in many cases never provided it.
Many of the individuals who advocate for ivermectin (and raise money doing it) have dubious professional behavior: Simone Gold, ER doctor & the founder of American's Frontline Doctors, was arrested by the FBI for taking part in the Capitol Attack on January 6. Gold pled guilty and is awaiting sentencing.
FLCCC’s leadership has also been described as “fringe": Paul Marik, intensivist & founder of FLCCC, was recently disciplined for prescribing opioids and other controlled substances to people who were not his patients. Marik previously claimed to have cured sepsis with vitamin C infusions. When this was disproven by multiple large RCTs he claimed that big pharma was suppressing the cure for sepsis. Marik has since had his clinical privileges suspended, unsuccessfully sued his employer, and then resigned. He no longer appears to practice medicine. Pierre Kory, another intensivist & the president of FLCCC, claimed that ivermectin was a "miracle cure" in his testimony before congress. He lost/left three critical care jobs in the last year and now sells ivermectin prescriptions online for $1250; his only source of income appears to be prescribing ivermectin.
Obviously the behavior of individuals doesn’t alter the efficacy of ivermectin, but it speaks to the character, credibility, and potential motivations of those who support it.
Conclusion: Ivermectin isn’t so extraordinary
Extraordinary claims require extraordinary evidence, and the claim that a repurposed medication miraculously both prevents and cures a fatal disease is quite extraordinary.
On close scrutiny the in vitro data and clinical trials do not support the use of ivermectin, which is why no reputable organization recommends it. The story isn’t over as there are more clinical trials in progress, but based on what we know so far, it doesn’t look promising for this “miracle cure.”
Grand Rounds Lecture: Debunking Ivermania
I recently gave a Grand Rounds Lecture summarizing much of the content above. You can watch a recording of the lecture, click through or download my slides here.

10/15/2021 Grand Rounds Lecture: Debunking Ivermania
Revision History
9/30 original post
10/4 updated to include new coverage about ivermectin in Brazil
10/8 updated to include evidence that Niaee et al study contains data irregularities
10/15 added video & PPT from my Grand Rounds Lecture: Debunking Ivermania
11/8 added ITECH trial results (another negative trial of ivermectin)
11/15 added retractions of Hill et al & Kory et al meta-analyses
11/26 added section on “Ivermectin didn’t save Japan”
12/21 added details about consequences for doctors spreading disinformation, edits for clarity in Japan section, added link to data for COVID cases in Japan
2/22 added more details about under-reporting of deaths in Uttar Pradesh, added link to newly published I-Tech trial
3/22 added more details about ivermectin grifters